

Shared Decision Making in Palliative Care: How Research Informs Practice for Case Management
BY ELLEN FINK-SAMNICK, DBH, MSW, LCSW, ACSW, CCM, CCTP, CRP, FCM
Case managers strive to provide quality-driven intervention to patients living with serious, life-limiting, and terminal conditions. These patients frequently face complex treatment choices that involve weighing the potential benefits of interventions against their impact on comfort, independence, and overall quality of life. Yes, successful care delivery is dependent on four critical elements: a research-informed palliative care process that encompasses shared decision-making and interactional communication.
Palliative care is an active, holistic approach used for individuals experiencing serious health-related suffering due to serious illness. Its intrinsic goal is to enhance the quality of life for patients, families, and caregivers by addressing physical, psychological, social, and spiritual needs (Radbruch et al., 2021). Pain control, maintaining independence, and spiritual or religious considerations may need to be processed. The patient or their family may want to avoid emergency department admissions or prolonged hospitalizations.
Shared decision-making is an essential phase of the communication pathway and embedded in serious illness treatment processes (Hoque, 2024; Montori et al., 2023). This interactional process provides a vehicle to honor both the provider’s expertise and the patient’s right to be fully informed of all care options, and their potential harms and benefits. Health care decisions are collaboratively defined through consideration of the best scientific evidence available, as well as the patient’s values and preferences. Yet well-intended practitioners can frequently find themselves at cross purposes with the patients and families they treat. The basic premise for the provision of health care implies there is an illness, treatment, and subsequent improvement in health, a return to wellness or recovery from injury. However, this perspective is more applicable when palliative care becomes part of the treatment equation.
Effective case management practice relies on the crucial tool of communication, which is a fundamental competency of the profession (Treiger, 2020). Verbal, non-verbal, and adaptive communication methods support shared decision-making, align care with patient values, mitigate misunderstandings, and foster compassionate, coordinated care throughout the course of any serious illness. Bi-directional communication involves clear, informative, and interactive engagement from patients, families, and interdisciplinary team members to comprehend the goals of care, treatment options, and patient preferences.
Research is a professional obligation in case management (Tahan, 2025). It is among the vital pillars of the profession that fuses the successful outputs of communication, shared decision-making, and palliative care to deliver successfully navigated conversations. Integrating evidence-based research in these critical elements of care provides case managers with the tools and frameworks they need to make informed, patient-centered decisions that align with individuals’ goals, values, and preferences. This process empowers all vested decision-makers in the treatment plan, while facilitating an efficient and effective care delivery process. This article will cite the current research to drive robust and successful case management communication on shared decision-making in palliative care.
EVIDENCE-BASED FOUNDATIONS OF SHARED DECISION MAKING
Considerable research anchors the seminal models, clinical pathways, and practice frameworks developed for shared decision making. Each of these crucial resources is leveraged by EBR that validates successful outcomes for greater patient engagement, higher patient, caregiver, and family satisfaction (Alanzi et al., 2024; Baik et al., 2019; Elwyn et al., 2012; Fink-Samnick, 2016; Galletta et al., 2022, Godfrey et al., 2024).
The seminal Three-Talk Model by Elwyn et al. (2012) defined a three-phase bi-directional consecutive communication process to guide practitioners in their serious illness conversations with patients and their families: choice talk, option talk, and decision talk. Each phase denotes a deliberate collaboration among parties allowing for exploration of the diagnosis and prognosis, review of all treatment alternatives with their benefits and consequences, and culminates in a decision to align with the cultural, spiritual, and other values of each patient.
The model was enhanced by Fink-Samnick (2016) with an additional fourth step for case managers known as “touch-back”. That final step accounts for the fluid nature of these often demanding decisions and provides all involved parties an equal opportunity to review where dialogues end and define further information required to keep the decision process advancing forward. This can become an optimal space for case managers to step in and best support the definition of next steps. The four-step model for case management appears in Figure 1.
Figure 1 Four-Step Model for Case Management
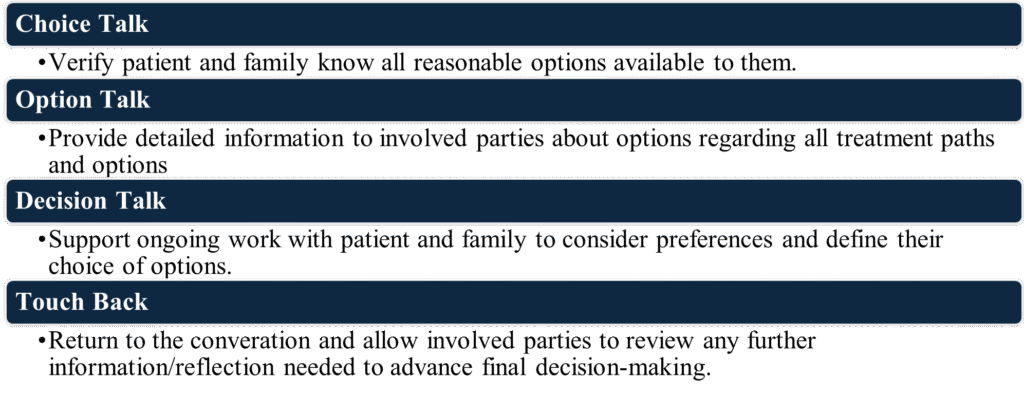
Adapted from Ellwyn et al., 2012 by Fink-Samnick (2016)
Autonomy and patient self-determination are primary ethical obligations by case managers. To do no harm is another of the workforce’s most sacred professional obligations. Studies show that when patients are actively involved in decision making, they are more likely to understand their condition, adhere to treatment recommendations, and feel satisfied with their care (Alanzi et al., 2024; Baik et al., 2019). Respect for self-efficacy in palliative care yields greater attention to the patient-centric care processes endemic to quality shared decision-making models (Elkefi & Asan, 2023).
Patients who participate in shared decision making often choose care approaches that prioritize comfort, dignity, and quality of life (Galletta et al., 2022; Godfrey et al., 2024). Patients admitted to cardiac intensive care unit (CICU) and their treating clinicians often process arduous decisions about aggressive or life-sustaining therapies. Pain control, maintaining independence, spiritual or religious considerations may need to be processed. The patient or their family may want to avoid emergency department admissions or prolonged hospitalizations. Case managers help ensure that care plans remain aligned with the patient’s priorities throughout the course of illness, by grounding treatment decisions in these personal values. For many individuals with serious illness, this may mean focusing on symptom management, maintaining independence, or spending the most meaningful time remaining with loved ones rather than pursuing aggressive medical interventions.
RESEARCH-INFORMED COMMUNICATION AND SHARED DECISION-MAKING
Effective communication is among the most important components of shared decision-making, and research has significantly shaped best practices in this area. Palliative care research highlights that communication should be clear, compassionate, and tailored to the patient’s level of health literacy and emotional readiness and is validated across the literature.
Tark et al. (2023) conducted a systematic review to identify and characterize conceptual and theoretical frameworks used in palliative and end-of-life care research. The authors searched four databases (2010–2021) and identified 44 eligible studies encompassing over 33,000 participants. Most of the studies introduced newly developed frameworks in the context, while others modified or applied existing models. Eight conceptual orientations were identified, reflecting perspectives such as patient, system, and patient–provider interactions. Nearly half of the frameworks aligned with only one domain of the National Consensus Project’s Clinical Practice Guidelines for Quality Palliative Care (2018). For those unfamiliar with this resource, it provided an interdisciplinary framework for delivering comprehensive palliative care across the lifespan and across care settings. The review concludes that greater integration of comprehensive frameworks is needed to strengthen methodological rigor and guide interdisciplinary palliative care research.
Other studies have shown that patients and families often struggle to understand complex medical terminology, conceptual terminology, or prognostic information (Rabben et al., 2024). Patients and their clinical teams can often use differing terminology to explain palliative care, which prompts further confusion with fully understanding the concept and its application to their clinical reality.
Health literacy also factors into this theme. Patients with limited health literacy experience communication challenges in comprehending palliative care dialogues with providers (Rhoodbeen et al., 2021). The intense emotions and vulnerability imposed by a hospitalization may grossly impact a patient’s ability to obtain, understand, process, and apply information. Their understanding further deteriorates when patients are further stressed by limited comprehension of their health status or provider overreliance on jargon. Team members can become frustrated and present as insensitive to the patient’s need for time, individualized attention, or other aspects reflective of truly patient-centric care (Rhoodbeen, et al., 2021).
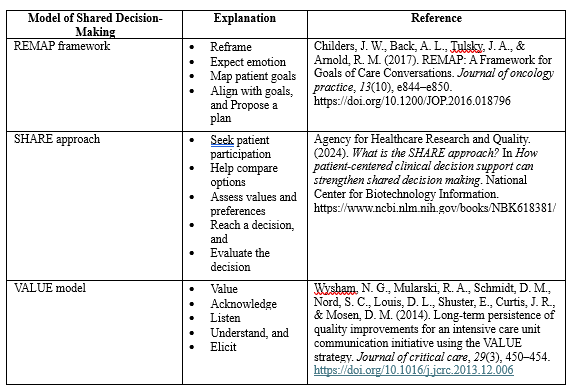
Work by Godfrey et al. (2024) explored models used in Intensive Care Units (ICUs) that employ plain language, visual aids, and structured conversation models. All models support the translation of clinical information into understandable terms that encompass four key domains:
- Communication strategies and conversation aids: Structured clinician- and patient-facing tools to promote shared decision-making dialogues
- Education interventions: Communication skills training focused on end-of-life and palliative decision-making
- Decision aids: Support interventions to prepare patients to participate in shared decision-making
- Family, multidisciplinary, and consultative support: Interventions to involve various decision-makers in the care process
Case managers may use these research-based communication techniques to ensure that patients fully understand their diagnosis, treatment options, and potential outcomes. They support patient self-efficacy and autonomy in articulating what matters most in the context of their quality of life. Examples of these models appear in Table 1.
DECISION AIDS AND EVIDENCE-BASED TOOLS
A variety of practical, research-based tools now support shared decision making in palliative care. These include symptom assessment scales, decision aids, screening instruments, and structured conversation guides that help patients and providers explore treatment options collaboratively.
Validated assessment tools allow case managers to gather objective data on symptom burden, functional status, psychological distress, and decision-making capacity. This information helps guide discussions about appropriate treatment pathways and supportive services. For example, symptom assessment instruments can help identify uncontrolled pain, fatigue, or anxiety that may influence a patient’s treatment preferences (Godfrey et al., 2024; Gonclaves et al., 2025).
Decision aids developed through research provide visual or written explanations of treatment choices, including potential benefits, risks, and expected outcomes (Godfrey et al., 2024). These tools are particularly valuable in palliative care, where treatment decisions may involve complex considerations about life-prolonging therapies, hospice care, or comfort-focused interventions. By presenting information in a structured and understandable format, decision aids empower patients and families to actively participate in care planning.
INTERDISCIPLINARY COLLABORATION AND CARE COORDINATION
Research in palliative care consistently demonstrates the importance of interdisciplinary collaboration. Palliative care teams typically include physicians, nurses, social workers, chaplains, therapists, and case managers, all working together to address the multifaceted needs of patients and families.
(Moreo et al., 2023) spoke to the unique role case managers place within this interdisciplinary team. Case managers often find themselves as the translators of complex medical information, helping patients and families understand treatment options while ensuring that their voices are heard during care planning discussions. Mota et al. (2022) looked at how case management optimizes care coordination for patients and their families during the palliative care process. This extends to integrating communications among team members and involved members of the immediate family. Use of shared decision making during these interactions ensures that patient preferences are consistently reflected in the plan of care.
Studies have found that case management facilitation of shared decision making for patients with complex chronic conditions within interdisciplinary teams yields improved care coordination and fewer unwanted interventions (Hudon & Kessler, 2023; Karam et al., 2021; Moreo et al., 2023). This collaborative approach helps ensure that care decisions remain consistent with the patient’s goals, given how rapidly their clinical circumstances change.
CULTURAL COMPETENCE IN SHARED DECISION MAKING AND PALLIATIVE CARE
Current research highlights the critical intersection of cultural competence, shared decision-making, and palliative care in improving patient-centered outcomes. Cultural beliefs and traditions strongly influence how individuals perceive illness, suffering, medical interventions, and end-of-life care (Hira et al., 2025). Some patients may prefer individual autonomy in decision-making, while others rely on family-centered or community-based decision processes.
Cultural beliefs and values strongly influence perceptions of illness, death, communication preferences, and treatment choices at the end of life, making culturally responsive care essential in palliative settings. Montori et al. (2022) emphasized how shared decision-making supports culturally sensitive care by ensuring that treatment decisions reflect the patients’ cultural, spiritual, and family priorities. Emerging studies also demonstrate how practitioners with stronger cultural competence are better able to build trust, reduce disparities, and improve satisfaction with palliative care among diverse populations (Burke et al., 2023).
Qualitative research and population-based studies have helped identify how culturally responsive communication strategies that respect diverse values and traditions can facilitate advance care planning, including shared decision-making. Kim & Flieger (2023) noted how barriers can ensue when discordant views emerge between provider and patient, or there is dismissal of the patient or family’s individual perspectives altogether. Case managers are reminded of their ethical accountability to patients and families in this regard, and guidance of conversations that acknowledge cultural perspectives on illness, spirituality, and caregiving.
By incorporating culturally informed approaches, case managers help ensure that shared decision-making remains respectful and inclusive. This research-informed sensitivity strengthens trust between healthcare providers, patients, and families, ultimately improving the quality of palliative care.
CONTINUOUS QUALITY IMPROVEMENT THROUGH RESEARCH
Baik et al. (2018) explored the role of shared decision-making in shaping individual clinical interactions and fostering broader quality improvement initiatives within palliative care programs. Healthcare systems are increasingly utilizing research data to assess outcomes such as symptom management, patient satisfaction, caregiver support, and appropriate hospice utilization (National Consensus Project for Palliative Care, 2018; Rabben et al., 2024).
Case managers play a pivotal role in these efforts by documenting patient experiences, monitoring care outcomes, and actively participating in program evaluation initiatives. Through the analysis of research findings and outcome data, healthcare teams can identify avenues for enhancing communication, care coordination, and patient engagement.
Continuous quality improvement ensures that shared decision-making practices evolve in tandem with emerging evidence and evolving patient needs. When case managers actively engage with current research, they are better informed and equipped to provide the most compassionate, effective, and patient- and family-centric care possible.
CONCLUSION AND IMPLICATIONS FOR CASE MANAGEMENT
When shared decision-making and quality communication within palliative care are fueled by evidence-based research, case managers are provided an unyielding foundation that empowers them to effectively heed the Quintuple Aim. Evidence-based communication strategies, validated assessment tools, decision aids, and interprofessional collaboration all contribute to a structured, ethical, and compassionate approach to care planning.
The merging of these critical elements to clinical practice enhances the ability of case managers in skillfully supporting patients and families to navigate intricate healthcare decisions with enhanced clarity and confidence. Research-informed approach assure that treatment choices are not only grounded in clinical evidence but also align with the patient’s individual objectives, cultural values, and aspirations for quality of life.
Patient advocacy and autonomy are among the primary ethical tenets of case management practice (CMSA, 2022; Fink-Samnick, 2023). Application of evidence-based research advances shared decision-making in palliative care conversations provides patients and their families greater control over what is often viewed as an uncontrollable care trajectory. This action further heeds case management’s professional obligations by demonstrating keen attention to standards of practice, including:
- Ethics (D)
- Advocacy (E)
- Resource Management (G)
- Planning (L)
- Facilitation, Coordination, and Collaboration (M)
- Monitoring (N)
- Outcomes (O), and
- DEIB and Health Equity (Q).
The integration of research into palliative care practice enhances case management’s role in upholding dignity, ensuring comfort, and fostering meaningful patient engagement throughout the course of serious illness. Research-informed shared decision-making frameworks provide practical guidance on how to structure these conversations. They also prioritize transparency with this treatment process, which facilitates a balanced informed consent discussion that prioritizes the quality of life as defined by the patient and family.
REFERENCES
Alanzi, T. M., Alanzi, N., Majrabi, A., Alhajri, A. S., Alzahrani, L., Alqahtani, N., Alqadhibi, A., Alenazi, S., Alsaedi, H., Alghamdi, E., Bin Hamad, N., Habib, W., Alharthi, N. H., Alharbi, M., & Alyahya, N. N. (2024). Exploring Patient Preferences Related to Shared Decision-Making in Chronic Disease Management. Cureus, 16(9), e70214. https://doi.org/10.7759/cureus.70214
Baik, D., Cho, H., & Masterson Creber, R. M. (2019). Examining Interventions Designed to Support Shared Decision Making and Subsequent Patient Outcomes in Palliative Care: A Systematic Review of the Literature. The American journal of hospice & palliative care, 36(1), 76–88. https://doi.org/10.1177/1049909118783688
Burke, C., Doody, O., & Lloyd, B. (2023). Healthcare practitioners’ perspectives of providing palliative care to patients from culturally diverse backgrounds: a qualitative systematic review. BMC palliative care, 22(1), 182. https://doi.org/10.1186/s12904-023-01285-3
Case Management Society of America (2022, 2024). Standards of practice for case management; Author: Brentwood, TN
Elkefi, S., & Asan, O. (2023). The Impact of Patient-Centered Care on Cancer Patients’ QOC, Self-Efficacy, and Trust Towards Doctors: Analysis of a National Survey. Journal of patient experience, 10, 23743735231151533. https://doi.org/10.1177/23743735231151533
Elwyn, G., Frosch, D., Thomson, R., Joseph-Williams, N., Lloyd, A., Kinnersley, P., Cording, E., Tomson, D., Dodd, C., Rollnick, S., Edwards, A., & Barry, M. (2012). Shared decision making: a model for clinical practice. Journal of general internal medicine, 27(10), 1361–1367. https://doi.org/10.1007/s11606-012-2077-6
Fink-Samnick E. (2016). The Evolution of End-of-Life Care: Ethical Implications for Case Management. Professional case management, 21(4), 180–192. https://doi.org/10.1097/NCM.0000000000000159
Fink-Samnick, E. (2023). The Ethical Case Manager: Tools and Tactics, Blue Bayou Press
Fink-Samnick, E. (2025). Is Case Management’s Interprofessional Power Also Its Kryptonite?. Professional case management, 30(5), 187–189. https://doi.org/10.1097/NCM.0000000000000811
Galletta, M., Piazza, M. F., Meloni, S. L., Chessa, E., Piras, I., Arnetz, J. E., & D’Aloja, E. (2022). Patient Involvement in Shared Decision-Making: Do Patients Rate Physicians and Nurses Differently?. International journal of environmental research and public health, 19(21), 14229. https://doi.org/10.3390/ijerph192114229
Godfrey, S., Barnes, A., Gao, J., Sulistio, M. S., Katz, J. N., & Chuzi, S. (2024). Shared Decision-making in Palliative and End-of-life Care in the Cardiac Intensive Care Unit. US cardiology, 18, e13. https://doi.org/10.15420/usc.2024.03
Gonçalves, F., Gaudêncio, M., Rocha, A., Paiva, I., Rego, F., & Nunes, R. (2025). A Review on the Management of Symptoms in Patients with Incurable Cancer. Current oncology (Toronto, Ont.), 32(8), 433. https://doi.org/10.3390/curroncol32080433
Hira, V., Palnati, S. R., & Bhakta, S. (2025). Understanding the Influence of Culture on End-of-Life, Palliative, and Hospice Care: A Narrative Review. Cureus, 17(7), e87960. https://doi.org/10.7759/cureus.87960
Hoque F. (2024). Shared Decision-Making in Patient Care: Advantages, Barriers and Potential Solutions. Journal of Brown hospital medicine, 3(4), 13–15. https://doi.org/10.56305/001c.122787
Hudon, C., & Kessler, R. (2023). Integrating case management for patients with complex needs in the ground practice: the importance of context in evaluative designs. Health research policy and systems, 21(1), 9. https://doi.org/10.1186/s12961-023-00960-4
Karam, M., Chouinard, M. C., Poitras, M. E., Couturier, Y., Vedel, I., Grgurevic, N., & Hudon, C. (2021). Nursing Care Coordination for Patients with Complex Needs in Primary Healthcare: A Scoping Review. International journal of integrated care, 21(1), 16. https://doi.org/10.5334/ijic.5518
Kim, H., & Flieger, S. P. (2023). Barriers to Effective Communication about Advance Care Planning and Palliative Care: A Qualitative Study. Journal of hospice and palliative care, 26(2), 42–50. https://doi.org/10.14475/jhpc.2023.26.2.42
Montori, V. M., Ruissen, M. M., Hargraves, I. G., Brito, J. P., & Kunneman, M. (2023). Shared decision-making as a method of care. BMJ evidence-based medicine, 28(4), 213–217. https://doi.org/10.1136/bmjebm-2022-112068
Mota, L., Melo, R., Silva, C., Principe, F., Pereira, H., Alvarenga, M. Soares, S. (2022). Nursing case management in palliative care; Nursing Practice Today; https://doi.org/10.18502/npt.v9i3.10220
Moreo, K., Sullivan, S., Carter, J., & Heggen, C. (2023). Generating team-based strategies to reduce health inequity in cancer care. Professional Case Management, 28(5), 215–223. doi:https://doi.org/10.1097/NCM.0000000000000657
National Consensus Project for Quality Palliative Care. (2018). Clinical practice guidelines for quality palliative care (4th ed.). National Coalition for Hospice and Palliative Care. https://www.nationalcoalitionhpc.org/ncp
Rabben, J., Vivat, B., Fossum, M., & Rohde, G. E. (2024). Shared decision-making in palliative cancer care: A systematic review and metasynthesis. Palliative medicine, 38(4), 406–422. https://doi.org/10.1177/02692163241238384
Radbruch, L., De Lima, L., Knaul, F., Wenk, R., Ali, Z., Bhatnaghar, S., Blanchard, C., Bruera, E., Buitrago, R., Burla, C., Callaway, M., Munyoro, E. C., Centeno, C., Cleary, J., Connor, S., Davaasuren, O., Downing, J., Foley, K., Goh, C., Gomez-Garcia, W., … Pastrana, T. (2020). Redefining Palliative Care-A New Consensus-Based Definition. Journal of pain and symptom management, 60(4), 754–764. https://doi.org/10.1016/j.jpainsymman.2020.04.027
Roodbeen, R., Vreke, A., Boland, G., Rademakers, J., van den Muijsenbergh, M., Noordman, J., & van Dulmen, S. (2020). Communication and shared decision-making with patients with limited health literacy; helpful strategies, barriers and suggestions for improvement reported by hospital-based palliative care providers. PloS one, 15(6), e0234926. https://doi.org/10.1371/journal.pone.0234926
Rosca, A., Karzig-Roduner, I., Kasper, J., Rogger, N., Drewniak, D., & Krones, T. (2023). Shared decision making and advance care planning: a systematic literature review and novel decision-making model. BMC medical ethics, 24(1), 64. https://doi.org/10.1186/s12910-023-00944-7
Tahan, H. (2025). The Professional Case Manager’s Obligation Toward Advancing Research and Evidence-Based Practice. Professional Case Management 30(5):p 220-223, September/October 2025. | DOI: 10.1097/NCM.0000000000000822
Tark, A., Estrada, L. V., Stone, P. W., Baernholdt, M., & Buck, H. G. (2023). Systematic review of conceptual and theoretical frameworks used in palliative care and end-of-life care research studies. Palliative medicine, 37(1), 10–25. https://doi.org/10.1177/02692163221122268
Treiger T. M. (2020). Shared Decision-Making: A New Frontier for Case Management Leadership. Professional case management, 25(2), 56–76. https://doi.org/10.1097/NCM.0000000000000394
Wang, Y., Li, J., Yin, N., Huang, B., Shen, K., He, S., Yang, M., & Zhang, J. (2026). The effect of shared decision-making for critically ill patients: a systematic review and meta-analysis. Frontiers in medicine, 13, 1726976. https://doi.org/10.3389/fmed.2026.1726976
 Dr. Ellen Fink-Samnick, DBH, MSW, LCSW, ACSW, CCM, CCTP, CRP, FCM, is a distinguished author, educator, and thought leader who specializes in health equity, integrated care, interprofessional ethics, professional case management, quality improvement, and trauma-informed education and leadership. She is a faculty member, academic advisor, and IRB Coordinator for the Doctoral Program at Cummings Graduate Institute of Behavioral Health studies. Dr. Fink-Samnick actively participates in a diverse range of national leadership and consultant roles within the industry. Her extensive academic contributions include authorship of six scholarly texts, over 100 articles, and other valuable knowledge content. She is recipient of CMSA’s 2025 Case Manager of the Year Award, the CMSA Foundation’s 2025 Research Award (with colleagues), and recipient of CMSA’s 2016 Award of Service Excellence.
Dr. Ellen Fink-Samnick, DBH, MSW, LCSW, ACSW, CCM, CCTP, CRP, FCM, is a distinguished author, educator, and thought leader who specializes in health equity, integrated care, interprofessional ethics, professional case management, quality improvement, and trauma-informed education and leadership. She is a faculty member, academic advisor, and IRB Coordinator for the Doctoral Program at Cummings Graduate Institute of Behavioral Health studies. Dr. Fink-Samnick actively participates in a diverse range of national leadership and consultant roles within the industry. Her extensive academic contributions include authorship of six scholarly texts, over 100 articles, and other valuable knowledge content. She is recipient of CMSA’s 2025 Case Manager of the Year Award, the CMSA Foundation’s 2025 Research Award (with colleagues), and recipient of CMSA’s 2016 Award of Service Excellence.

