
Evidence-Based Assessments and Interventions Supporting Population Health
INTRODUCTION
As a follow up to the article and poster presentation on Sustainable Strategies to Prevent Health Care Worker Exodus, our Trinity Health ambulatory care management teams continue to assess and trend average patient risk scores. Frequently, care management teams are evaluated based on financial returns on investment (ROI), and there has been much discussion related to regression to the mean. Providing real-time risk assessment ensures our care managers are engaging the right populations and focusing on the patient’s individual area of risk. As we know, the underlying causes of a condition can be much more than condition burden or symptoms. Social needs and untreated or undertreated conditions are common contributors to poor health.
As you may recall, Trinity Health collaborated with the Case Management Society of America (CMSA) to provide training of the ambulatory care management teams through the CMSA Integrated Case Management (ICM) program. Ambulatory care managers trained in an integrated approach assess risk in the four domains of health: biological, psychological, social and health system. They use these assessments to develop and create a shared person-centric plan of care. The ICM training provides advanced assessment training, identifying the person’s experiences, concerns, and what is contributing to poor health. This results in a plan of care that focuses on what is most important to the person.
Trinity Health leadership’s commitment to personalized care delivery supports our mission of being a transforming and healing presence within the communities we serve. Using evidence-based clinical practice and resources ensures our patients/members are the center of our care, and partnership throughout the continuum helps ensure our members achieve their health goals.
PURPOSE
The purpose of this quality improvement initiative is to determine whether additional care management education and membership in a national organization, the Case Management Society of America (CMSA), would increase retention, decrease turnover and decrease average risk scores by age and primary diagnosis within our populations managed by our ambulatory care management teams.
PROBLEM STATEMENT
The ambulatory care managers needed a different solution for onboarding, orientation and ongoing training to decrease turnover and ensure a high degree of competency to increase patient engagement, thereby influencing and decreasing patient risk. The health system cost of turnover is calculated as equivalent to a 12-month CM salary to train inexperienced staff.
Care managers are key members of the care team, supporting member care, transitions of care, care coordination, education, and are well-positioned to improve the member experience, decrease cost, decrease risk and improve patient outcomes. To ensure that we are the employer of choice, we need to recruit high quality applicants, effectively train to ensure competency and retain our CM nurses and social workers.

LITERATURE REVIEW
For care management leaders, the efficacy of our care management programs depends on ensuring standard evidence-based interventions that engage the patients we serve. As referenced by the Agency for Healthcare Research and Quality (AHRQ, 2014), “the literature review found evidence of care management interventions improving outcomes across all diseases successfully.” In a literature review reported by AHRQ, in-person and telephonic care management along with patient activation and self-management education have demonstrated an improvement in utilization, clinical outcomes, processes, cost measures and medication administration.
Doody and Doody (2012) discuss the importance of having transformational leadership that influences, inspires and motivates, ensures intellectual stimulation and provides for individual consideration. Adaptive transformational leadership supports employee engagement and satisfaction, further causing a ripple effect of patient satisfaction and retention. Therefore, as leaders engaging our teams, educating and creating standard work is fundamental.
INTERVENTIONS
CMSA’s philosophy aligned with Trinity Health’s in achieving goals for improving health outcomes for the population’s services and participation in advanced payment models. CMSA’s Integrated Case Management Program (ICM) training teaches care managers how to engage members, create trusted relationships and perform a comprehensive assessment providing whole person care, and the development of a care plan (CMSA, 2020).
Each ambulatory care manager including nurses and social workers along with their leaders received ICM training and have CMSA membership providing access to CMSA’s library, tools and webinars. Care managers collaborating with complex patients have a goal to follow five patients for 12 months, recording baseline ICM risk scores and providing quarterly updates on risk scores using RedCap database for the participants within the Medicare Shared Savings Program.
PROJECT AIMS
The aims of this quality improvement project were to
- Increase competency and skills by training 90% ambulatory care managers and their leaders through the Integrated Case Management course by June 31, 2023.
- Increase access to educational events and training tools through the CMSA membership library.
- Decrease ambulatory care manager turnover rates.
- Increase the retention of ambulatory care managers.
- Improve the risk scores of patients being care managed.
THEORETICAL FRAMEWORK
The Neumann system model provides a frame of reference for evaluating and addressing health conditions across distinctive settings. The model supports a holistic framework supporting the use of clinical tools to guide assessment of individuals, families, communities and organization to influence clinical practice. “Nurses evaluate the effectiveness of their interventions based on the degree to which clients met their goals” (Whetsell, Gonzalez, & Moreno-Fergusson, 2015).
The ICM model provides for a standard way to identify health risks and health needs using the biological, psychological, social and health system domain. Through the evaluation of historical, current state and vulnerabilities, the CM can better identify areas of risk and priorities when developing a patient-centered care plan.
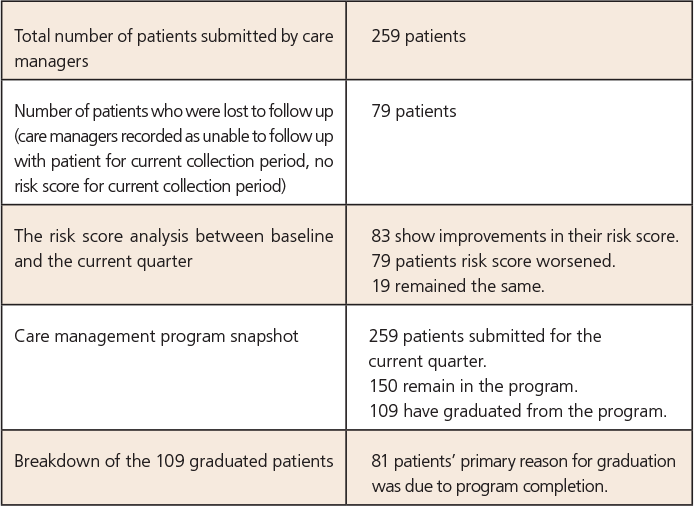
Clinical results as of the third quarter of the study findings include:
METHOD/PROJECT DESIGN AND INTERVENTIONS
The quality improvement project is a prospective, mixed model including self-study and interactive face-to-face virtual training. The program provides multiple strategies to engage patients, risk stratify, and developed a patient-centered care plan to decrease risk and improved well-being. The interventional design included pre-work of reading the CSMA ICM book, three to four hours of online presentations, and three four-hour (half-day) training sessions. Each cohort had a maximum of 25 people to ensure time for individualized and group interaction in reviewing case studies. The audience included a combination of nurses, social workers and CM leaders from the ambulatory care management teams that support the advanced payment models in the clinically integrated networks across the country.
DATA AND ANALYTICS
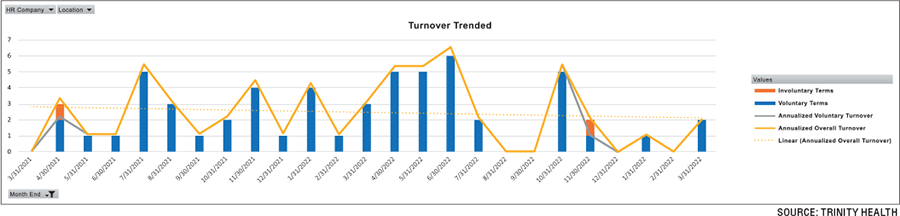
Colleague results show turnover data trends for the ambulatory care management teams include a 25-month look back. As of May 11, 2023, the percentage of staff turnover within less than one year of recruitment is currently 21.82%. There are 55 hires of less experienced care managers. As noted in the graph on page 18, we have significantly decreased our turnover rates since the beginning of this intervention in June 2022. The predominate reason cited for turnover was personal reasons and new jobs.
In summary, there were a total of 16 cohorts (319 care managers trained) with a maximum of 25 CM per cohort training session (June 2022 – April 2023). Current retention rate for all cohorts is an overall 96%.
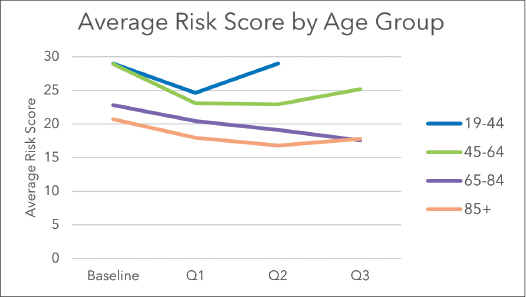
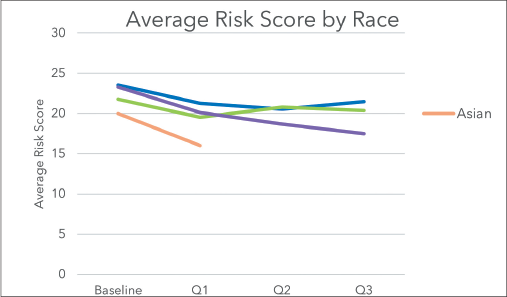
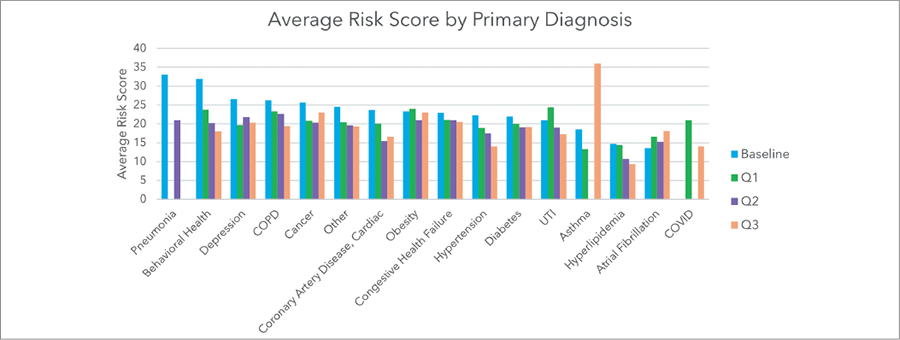
As noted in the graphs on page 19, the average risk scores for the third quarter of the study were trended and quantified by age group, race and diagnosis.
The Epic risk score for hospital admission and ED visit was compared to the ICM-CAG risk score. Although there was no clear and consistent correlation between Epic risk score and the ICM-CAG total risk score, it is worth noting that only patients with a “high” Epic risk score received a total risk score of 40 or higher (range is 0-60 for the study sample). Of note, the study was carried over two performance years. Medicare Shared Savings Program attribution may also factor into the interventions.
CONFLICT OF INTEREST AND PERMISSIONS
There are no conflicts of interest. The QI project aligns with the Catholic health system mission, vision and strategy and supports patient-centered relationship-based care through assessment and patient engagement leveraging motivational interviewing. Providing evidence-based learning opportunities for care management leaders and colleagues promotes safe care and continuous quality improvement.
LIMITATIONS
Limitations include the timeline of the intervention and the need for continued monitoring and evaluation. There are three clinically integrated networks that were not included in the turnover and retention graphs from the System Office Human Resource data.
SUMMARY AND CONCLUSIONS
The ambulatory care management team continues to be very appreciative of the CMSA ICM training and membership. Creating team expectations and building upon knowledge and skills supports our goal to continue to advance CM engagement and competency. Leveraging a national system approach facilitates overall improvement in interventions, care plans and patient care delivery.
Recommendations include continued monitoring of turnover and retention rates to ensure sustainability. Future state needs include evaluation of the efficacy within CM interventions to ensure decrease and/or mitigate risk.
ACKNOWLEDGMENTS
The author thanks Rebecca Perez, MSN, RN, CCM; Michele Lee, Amy Black, Tom O’Grady, Sheila Johnson, MBA, RN; Emily Brower, MBA; Gay Landstrom, PhD, RN, NEA-BC, FACHE; Ryan Berger, Michelle Fitch, and the CM leaders and national teams for their commitment and support of the training and quality improvement initiative.
REFERENCES
Agency for Healthcare Research and Quality (2014). Section 8: The Care Management Evidence Base. Retrieved from: https://www.ahrq.gov/patient-safety/settings/long-term-care/resource/hcbs/medicaidmgmt/mm8.html
Cowden, T., Cummings, G., Profetto-McGrath, J. (2011) Leadership practices and staff nurses’ intent to stay: a systematic review. Journal of Nursing Management 19(4):461-77. doi: 10.1111/j.1365-2834.2011.01209.x
Doody, O. & Doody, C.M. (2012). Transformational leadership in nursing practice. British Journal of Nursing 21(20):1212-4, 1217-8. doi: 10.12968/bjon.2012.21.20.1212
Duru, D.C., & Hammoud, M.S. (2022). Identifying effective retention strategies for front-line nurses. Nursing Management, 29(1):17-24. doi: 10.7748/nm.2021.e1971
Fraser, K., Perez, R., Latour, C. (2018). CMSA’s integrated case management: A guide for case managers by case managers. Springer Publishing Company.
Whetsell, M. V., Gonzalez, Y. M., & Moreno-Fergusson, M. E. (2015). Models and theories focused on a systems approach. In J. B. Butts & K. L. Rich (Ed.), Philosophies and theories for advanced nursing practice 1st ed., pp. 407-434. Jones and Bartlett Learning.
Image credit: UUGANBAYAR/SHUTTERSTOCK.COM



