

Care Management Partnership with Community Health Workers Is Leading to Greater Health Equity
For the past three years, Trinity Health’s Clinically Integrated Networks (CIN), Community Health & Well-Being (CHWB) departments and the Medical Groups (THMG) have engaged in a national strategy for reducing preventable hospitalizations among Medicare Shared Savings Program (MSSP) beneficiaries with a special focus on our vulnerable dually enrolled (Medicare/Medicaid) population. Nationally, patients who are dually enrolled are more likely to experience poverty, have disabilities and be part of a racial and/or ethnic minority. Shared accountability and key performance indicators (KPIs) among the CINs, THMG and CHWB teams with a clinical and social care focus were integral to the success of this strategy.
BACKGROUND
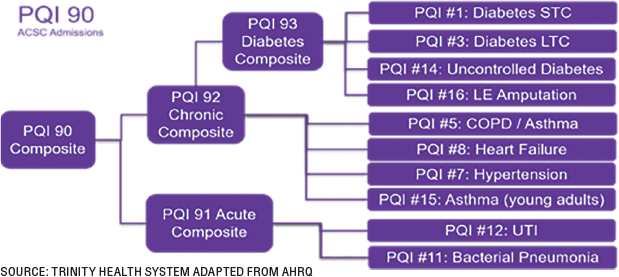
Preventable hospitalizations have been defined by the Agency for Healthcare Research and Quality (AHRQ) as specific conditions called ambulatory care sensitive conditions (ACSC). The conditions have the potential for good control through outpatient care and should rarely require hospitalizations. When someone is admitted to the hospital because of an ACSC, it is considered a preventable hospitalization. The AHRQ measure known as Prevention Quality Indicator 90 (PQI90) is comprised of multiple chronic conditions. The list of preventable conditions is identified below.
The primary driver of preventable hospitalizations nationally has been heart failure. Focused multidisciplinary reports were created and included claims and clinical data to inform the outreach initiatives related to guideline directed medication therapy (GDMT), health-related social needs and engaging patients to proactively schedule primary care visits.
STRUCTURE
The ambulatory care teams include care managers (nurses and social workers), pharmacists, community health workers and provider partnerships. Bringing these teams together and facilitating their understanding of each other’s roles were foundational. Meetings included care conferences, town halls, discipline-specific affinity meetings, structured education sessions and ministry progress and action planning meetings with executive leaders.
A Motivational Interviewing for Heart Failure program was designed with continuing education credits to support all members of the care teams. The education sessions were four hours in length and covered medication therapy and how to best support patient engagement and self-management through motivational interviewing. The structured breakout sessions with case studies helped all the attendees better understand each other’s roles and perspectives.
Key focus areas for the care managers include: 1) establish a chronic condition primary care office visit cadence, 2) create a patient-centered plan of care and 3) perform root cause analysis (RCA) (hospitalization is considered a system failure). Community health workers (CHWs) focus on conducting outreach, performing social needs screening, facilitating connection to community resources, conducting home visits and serving as cultural brokers between vulnerable patients and their providers. The teams refer to each other and co-manage patients based upon clinical and social needs. Ongoing care conferences between the community health workers and care managers have created great partnerships between the teams.
COLORECTAL CANCER SCREENING
Trinity Health’s 2022 MSSP data demonstrated a disparity in colorectal cancer screening rates between the overall attributed patient population (56.2%) and the Black, lower-income subset of these patients dually enrolled in Medicare and Medicaid (44.1%). This is unsurprising given the proven impact of poverty and racism on health outcomes, but it is especially concerning given that colorectal cancer incidence is 20% higher, and mortality is 40% higher, among Black Americans as compared to most other racial and ethnic groups (American Cancer Society, 2022, 2023).
In mid-2023, Trinity Health’s board of directors requested a special outreach project to improve colorectal cancer screening rates among these Black dually enrolled patients. CIN care teams of nurse care managers (CMs), social workers (SWs) and community health workers (CHWs) were educated on the disparity’s significance, provided with patient lists, and scripting. Then, leveraging their collaborative relationship, CMs conducted chart reviews to confirm each patient’s appropriateness for outreach, and CHWs called patients in the fall of 2023 to discuss the importance of colorectal cancer screening, address any unmet health-related social needs creating barriers, and to offer a warm hand-off to the patient’s primary care provider office for the next steps in obtaining screening through a three-way call or electronic medical record messaging function.
CHWs spoke with 53% of the patients they attempted to contact despite using the notoriously low yield “cold call” approach and made a warm hand-off to the providers of 88% of the patients they reached. However, less than 1% of the patients CHWs called had completed a screening as of four months post-outreach. These results indicate that CHWs are effective in engaging patients in vulnerable populations. The results also indicate that a single telephone discussion does not result in immediate acceptance of screening services, even when a warm hand-off to providers has occurred. Many of the participating CHWs reported a desire to continue following up with patients but were not able to do so within this project’s limits. While this project was not successful in closing the care gap, disseminating information about this project to medical, community health and administrative leaders across the Trinity Health system did raise awareness of the opportunity to employ interventions with the express purpose of narrowing a racial/ethnic or socioeconomic disparity in health outcomes. This helped inspire a systemwide initiative to address racial disparities in hypertension control experienced by the Black patient population with both medical and social support, launching in 2025.
WORKFLOWS
Foundational to the program was establishing workflows and developing prioritized outreach lists for the dually enrolled members. CHWs focused on patients experiencing poverty and other vulnerabilities based on home zip code, social needs screening results and inability to pay for medications. CHWs work to build trust, facilitate communication and serve as a cultural broker between vulnerable patients and their providers/care team through phone calls, home visits and in-office encounters. CHWs reinforce the plan of care and provide basic health education.
Depending on the care needs, patients are co-assigned to a CM as needed to ensure holistic care including medical and social support. Weekly case reviews and case presentation helped to build the relationships between colleagues. We found it was important to build both the credibility and confidence of our CHWs and focus on top of licensure practices for all members of the clinical teams. Leadership presence at the care conference helped to stress the importance of the work and provided for role modeling of expected behaviors. Standardized CHW training and an internal certification program also helped clinical colleagues to feel comfortable in the CHWs’ preparation for the role.
Comprehensive social needs screening helped to clearly identify needs, and the interventions required to improve outcomes. The teams used the Community Resource Directory powered by Find Help, a national online database of free and low-cost community resources, to help identify resources and make referrals.
OUTCOMES
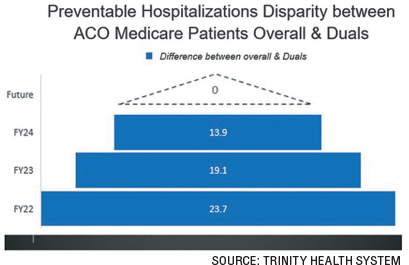
Dually enrolled patients are known to be a high cost, high utilization group, and it can become routine to see worse health outcomes and higher rates of undesirable utilization, such as a preventable hospitalization, among this group. Providing equitable care, however, means it is incumbent on us to identify and provide the additional support needed by this group to achieve outcomes that are as good as those found among other patient groups. The collaboration between CMs and CHWs and greater identification and intervention for patients’ health-related social needs were intended to do just that. As of April 2024, the disparity between the overall ACO rate of preventable hospitalizations and that of the patient subset dually enrolled in Medicaid has narrowed by 41% since 2022. In at least one chapter of Trinity Health’s MSSP, the rate for dually enrolled patients is almost the same as that of the overall patient population. This is the outcome we seek across our system. Intentionality and prioritization in telephonic outreach efforts drives greater health equity for the dually enrolled patients within the Medicare ACO program.
LESSONS LEARNED
- Establish a trusted relationship.
- Evaluate patients holistically, e.g., medical, social, spiritual.
- Perform social needs screening to identify access to food, living environment, cellphone, financial stability, safety, support systems, etc.
- Identify medical needs along with medication resources and storage, e.g., refrigeration needed for insulin.
- Engage in education, facilitate self-management, and coordination of care.
- Assist with and/or accompany to appointments, community resources such as Department of Social Services to complete need applications, e.g., Supplemental Nutrition Assistance Program (SNAP), Supplemental Security Income (SSI).
- Assist with identifying permanent housing and achieving financial stability.
CONCLUSION
In summary, the investment in building multidisciplinary care team relationships and integrating the care teams has led to a more comprehensive approach in caring for our patients. Shared accountability through national KPIs brought teams together and created a shared urgency to improve our current care delivery models. As a result, our collaborative team efforts are improving health equity in the MSSP attributed beneficiaries.
REFERENCES
Agency for Healthcare Research and Quality (2020). Statistical Brief #259. Healthcare Cost and Utilization Project (HCUP). Retrieved from: https://hcup-us.ahrq.gov/reports/statbriefs/sb259-Potentially-Preventable-Hospitalizations-2017.jsp.
Agency for Healthcare Research and Quality (2023). Quality Indicator User Guide: Prevention Quality Indicators (PQI) Composite Measure, c2023. Retrieved from: https://qualityinidcators.ahrq.gov/downloads/modules/PQI/V2023/PQI_composite_measures.pdg.
American Cancer Society. Cancer Facts & Figures 2023. Atlanta: American Cancer Society; 2023.
American Cancer Society. Cancer Facts & Figures for African American/Black People 2022-2024. Atlanta: American Cancer Society, 2022.

, DNP, MSA, RN, CCM, CPHQ, FCM, serves as the director, System Population Health and Care Management for Trinity Health System, a multi-institutional Catholic healthcare delivery system spanning 25 states. In this role, Lisa collaborates with leadership and teams across clinical, business and community health domains to improve the health and well-being of our patient populations. Lisa is passionate about creating standard evidence-based programs that support high quality patient care delivery systems. Lisa currently serves as president for the CMSA-Detroit Chapter and is a member of the Editorial Board of CMSA nationally. Lisa also serves as co-chair of the Epic Care Management Advisory Board.

, MPH, MBA, RN, scales initiatives to address the social influencers of health and patient social needs among populations experiencing poverty and other vulnerabilities. She is currently director of Social and Clinical Care Integration at Trinity Health, a non-profit healthcare delivery system spanning 26 states. Her experience includes critical care nursing, healthcare-community partnerships, disease prevention, healthcare access, value-based care and social care integration from local to national levels. Maureen received a BS in Nursing from Kent State University, MPH from the Johns Hopkins Bloomberg School of Public Health and a MBA from the Kellogg School of Management at Northwestern University.
Image credit: LIGHTSPRING/SHUTTERSTOCK.COM



