

Ensuring Positive Outcomes In Care Management
Perhaps the first step in looking at outcomes for care management, or any clinical program, is to identify the purpose of capturing outcomes. First, outcomes are captured in order to report to those invested in the service (boards, clients or program administrators) how effective or ineffective the service is. Funding decisions can be made based on these results. They will be determining if there is a benefit to providing this service to the members of the health plan. Perhaps the most significant reason for capturing outcomes, however, is to provide feedback to practitioners so that interventions can be adjusted. The regular review of outcomes and the timely provision of outcome information allows for adjustments in interventions and the ability to retest the impact.
Medical management programs like utilization, case and disease management were implemented primarily to impact utilization patterns and overall health-related costs. These programs gained prominence in the U.S. in the 1970s, 1980s and 1990s respectively. On a macro level, changes in these areas have been limited. For many, many reasons national trends in the areas of utilization and cost of care have not changed significantly since these programs were implemented.
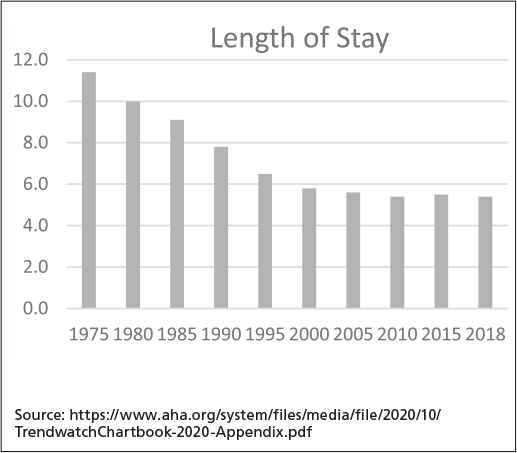
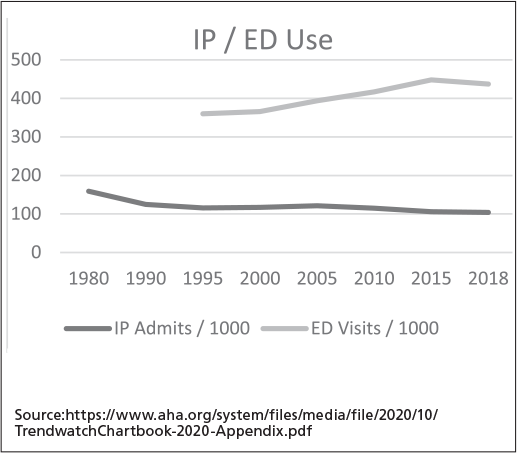
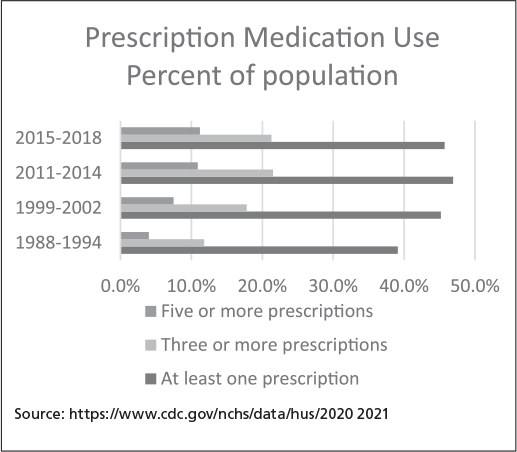
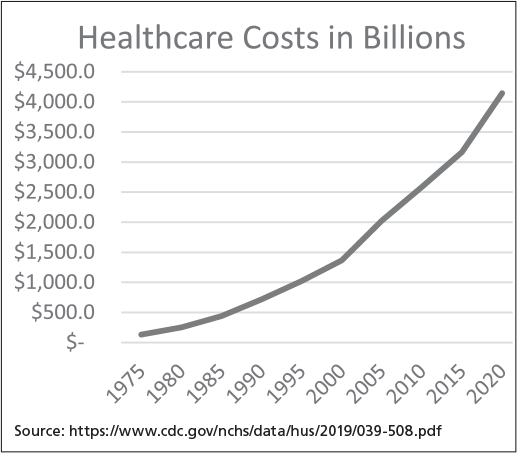
A sample of measurement of utilization and cost includes length of hospital stay, hospital admission rates, emergency room use, medication use and overall cost of care. Impacting these measurements is often seen as the responsibility of a medical management program. These graphs show variable changes over the years since these programs have been initiated in full. As seen, only hospital length of stay has shown any significant positive trend. The point of showing this is not to put the whole of responsibility on the failure of these programs but to rather point out that there are many factors that drive these patterns and that care management, as addressed below, can impact these outcomes by focusing not on these but on their contribution to factors that correlate to these patterns.
On a micro level, recent studies of the impact of care management on outcomes have shown conflicting results. Two examples of such conflict were shown in articles published in American Journal of Managed Care (AJMC) and Journal of American Medical Association Network (JAMA Netw). Both referenced complex care management programs, one for Medicaid enrollees and the other for Medicare ACO enrollees. The article published in AJMC in 2020 concluded that members in “CareMore Health” who were enrolled in the complex care program had lower total medical expenditure and fewer inpatient days than those enrolled in standard care. Other secondary outcomes were noted. However, the article published in JAMA Netw in 2019 concluded there was no statistical difference in the outcomes for those enrollees at the highest level of risk who received care management and coordination activities in comparison to those at the lower level of risk who also received care management and coordination.
One comprehensive meta-analysis in the Western Journal of Nursing Research (2018) on the impact of care management interventions on utilization measures concluded that there was evidence of care management positively impacting such utilization patterns as readmissions, length of stay, inpatient admissions and emergency room use. While they concluded care management interventions also impacted overall cost, the details showed that that result was mixed in the literature reviewed. The review, however, cited multiple issues with being able to point to exactly what impacted the outcomes. The authors stated that the review provided limited information on the exact interventions, the intensity of care management and the length of time in care management. These factors make it difficult to guide us in the best ways to impact the outcomes of interest.
These are all measures that can be impacted by so many variables; so, it can be difficult to determine what interventions can impact the outcomes that are seen as important to healthcare stakeholders and whether care management has any impact. The ability to consistently come to statistically significant conclusions about the impact of care management may be difficult, due to “the heterogeneity of CM programs in terms of what their intervention entails, the populations targeted, and the tools used to measure the results” (Cambridge Press).
But look at the areas where there are positive outcomes: adherence and satisfaction. If adherence to treatment guidelines can be considered one factor in the evidence of an individual engaging in their health, then highlighting the impact of an engaged individual in relation to positive outcomes would cause us to be hopeful. According to the CDC, “A growing body of evidence shows that people with higher patient activation (i.e., the knowledge, skills and confidence to become actively engaged in their healthcare) have better health outcomes,” and better health outcomes translate to lower healthcare costs.
One particular area of adherence that is significantly associated with positive health outcomes is medication adherence. Multiple articles and meta-analyses have shown that medication adherence for multiple conditions is significantly associated with lower hospital admissions, lower long-term mortality risk, fewer condition-specific complications and lower healthcare costs. According to a 2018 article published in BMJ Open, “the adjusted total cost of non-adherence across all disease groups ranged from $949 to $52,341 [per patient per year].” Multiple other research and meta-analyses report similar results. But, reportedly, care management, low co-pays and patient education with behavioral support all work to improve medication adherence and corresponding cost and clinical outcomes.
Patient satisfaction is also correlated with other positive clinical outcomes. In a 2016 AHRQ report, “Why Improve Patient Experience?”, the authors point out that a good patient experience is not only a positive outcome in its own right but is also associated with other clinical processes and outcomes. Some of these outcomes are better self-management skills, better adherence to medical advice and treatment plans and better overall health outcomes over time.
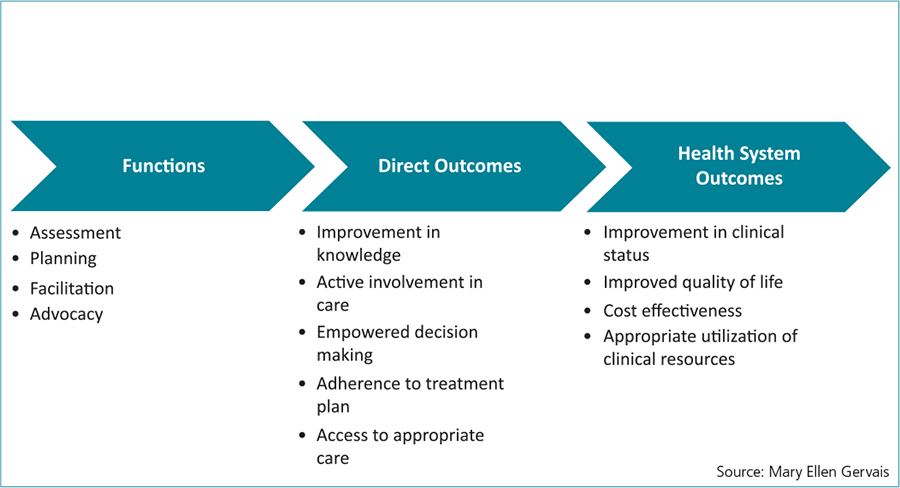
These positive impacts point to an outcome model that has been promoted and practiced for years in my practice and is still relevant to our model. The model was created by the Case Management Society of America (CMSA) and was called the Spectrum of Accountability. The model connects care manager functions with outcomes at different levels.
The significance of this model is the connection between the outcomes that can be directly impacted by care managers. As care managers work with members, they are able to activate them in the following ways:
- Improvement in knowledge of their condition, signs and symptoms of disease progression, self-management skills and management of the prescribed treatment plan. Improving knowledge is only the beginning of activation.
- Active involvement in self-management and lifestyle skills.
- Active participation in decision-making.
- Improved adherence to treatment plans, evidence-based guidelines for management of chronic conditions and lifestyle behaviors.
- In addition to these self-management skills, improved access to appropriate care is an outcome care management is equipped to address. Care managers are effective in removing barriers that are in the way of the member accessing care. Efficient access to care allows for the timely receipt of care.
As shown in the literature, as these outcomes are impacted, other outcomes (health system outcomes) are impacted for those who engaged with the care manager. With activation, clinical values are impacted, utilization of services is improved and the cost trajectory for these members is also improved. As satisfaction levels increase, a sense of well-being impacts the member’s quality of life.
The ability to show a positive trend in these areas in the entire population is a challenge due to factors like poor engagement with care management, limited number of people identified for care management and a very high care manager to employee ratio. But where would the trend for the members engaged with care management be had they not engaged?
CARE MANAGEMENT SPECTRUM OF ACCOUNTABILITY-ADAPTATION
How can the focus on these direct care management outcomes be promoted? The use of data is critical for this to be successful. Sources of data that are pertinent in this process include medical and pharmacy claims analyzed to provide risk and risk variable information; health risk assessment data; lab values; and care management assessment responses. From the analyzed data, care managers are guided using data-driven actions. These are prescriptive actions informed by comprehensively analyzed data.
Using the prescriptive direction driven by the data, the care managers work with the member toward achieving goals designed to address the issues and impact the direct outcomes of care management. Measurements of improved knowledge, improved adherence and active involvement in care are captured. Measurement of improved access to care is also captured. Progress toward achieving these goals is captured on a regular basis so that the care manager can tweak their interventions as they continue to support the member. The consistent availability of outcomes data is critical to ensuring ongoing attention to the data-driven actions and the direct outcomes associated with care management.
Health system outcomes are also critical to measure for these members so that we are able to show clearly the correlation between improvement in the direct outcomes of care management to improvement in the health system outcomes. In order to do this, cohorts of members with positive direct care management outcomes are created and integrated with available data. Claims-based data provides information on health system outcomes such as improved cost of care or cost effectiveness. It also provides information on appropriate utilization patterns comparing positive direct outcomes of care management to changes in hospital admissions and emergency room use. Improvement in clinical status is shown by integrating positive direct outcomes with outcomes related to changes in lab results over time.
Combining data-driven actions with direct outcomes of care management allows for regular tweaking of interventions so that positive outcomes are more likely. Integrating positive direct outcomes of care management with claims-based data and other data sources allows for the demonstration of the connection of these direct care management outcomes to the health system outcomes.
Measuring these types of outcomes regularly becomes a tool to ensure we are consistently tweaking our interventions to improve outcomes and becomes evidence of the value of care management. There is another value to being able to show what we can directly impact. As we can show that improvement in direct care management outcomes impacts outcomes of interest to the health system as a whole, we can advocate for the right level of care management resources for the populations we serve. We can engage in providing solutions for the typical poor engagement levels of members in care management programs. But more than all of this, we can bring our expertise in developing strategies to impact the larger population — not just those who we engage with. Since we know that improving these direct outcomes, helping to support people to be activated in their own health, will ultimately impact utilization and cost, we can bring strategies that we employ for those engaged with us to ways that these can be applied to the greater population. We can make meaningful use of technology to extend our reach to make the difference that is needed in the healthcare industry.

, PhD, RN, CCM, is president of EHG and an RN with more than 25 years of CM experience. Her PhD from Virginia Commonwealth University focused on the effective and meaningful practice of CM. Throughout her doctoral and master’s programs she studied outcomes research and measurements. She has presented and published on outcome- and data-driven CM. Dr. Gervais created a holistic, integrated model of care management that has resulted in major accomplishments for all, from the members themselves, to the payers, to the care managers. She has also been the key designer of an integrated care management system that guides professionals in evidence-based care management.
REFERENCES
Buja, A., Francesconi, P., Bellini, I., Barletta, V., Girardi, G., Braga, M., & Damiani, G. (2020). Health and health service usage outcomes of case management for patients with long-term conditions: A review of reviews. Primary Health Care Research & Development, Buja, A.
Cairns, C., & Kang, K. (2022). National Hospital Ambulatory Medical Care Survey: 2020 Emergency Department Summary Tables. NATIONAL CENTER FOR HEALTH STATISTICS. https://doi.org/10.15620/cdc:121911
Cutler, R. L., Fernandez-Llimos, F., Frommer, M., Benrimoj, C. S., & Garcia-Cardenas, V. (2018). Economic impact of medication non-adherence by disease groups: a systematic review. BMJ Open, 8(1), e016982. https://doi.org/10.1136/bmjopen-2017-016982
FastStats. (n.d.). Therapeutic Drug Use. https://www.cdc.gov/nchs/fastats/drug-use-therapeutic.htm
Han, E., Suh, D. I., Lee, S. H., & Jang, S. (2014). The impact of medication adherence on health outcomes for chronic metabolic diseases: A retrospective cohort study. Research in Social & Administrative Pharmacy, 10(6), e87–e98. https://doi.org/10.1016/j.sapharm.2014.02.001
Harrison, J. M., Oganisian, A., Grande, D., Mitra, N., Chhabra, M., & Chaiyachati, K. H. (2020). Econom Outcomes of Insurer-Led Care Management for High-Cost Medicaid Patients. The American Journal of Managed Care, 26(7), 310–316. https://doi.org/10.37765/ajmc.2020.43769
Health Literacy Research and Best Practices. (2021, August 16). Centers for Disease Control and Prevention. https://www.cdc.gov/healthliteracy/researchevaluate/patient-engage.html
How has U.S. spending on healthcare changed over time? – Peterson-KFF Health System Tracker. (2023b, February 7). Peterson-KFF Health System Tracker. https://www.healthsystemtracker.org/chart-collection/u-s-spending-healthcare-changed-time/#Total%20national%20health%20expenditures,%20US%20$%20Billions,%201970-2021
Joo, J. Y., & Huber, D. L. (2019). Case Management Effectiveness on Health Care Utilization Outcomes: A Systematic Review of Reviews. Western Journal of Nursing Research, 41(1), 111–133. https://doi.org/10.1177/0193945918762135
Ouayogodé, M. H., Mainor, A. J., Meara, E., Bynum, J. P., & Colla, C. H. (2019). Association Between Care Management and Outcomes Among Patients With Complex Needs in Medicare Accountable Care Organizations. JAMA Network Open, 2(7), e196939. https://doi.org/10.1001/jamanetworkopen.2019.6939
Section 2: Why Improve Patient Experience? (n.d.). Agency for Healthcare Research and Quality. https://www.ahrq.gov/cahps/quality-improvement/improvement-guide/2-why-improve/index.html
Viswanathan, M., Viswanathan, M., Golin, C. E., Jones, C., Ashok, M., Blalock, S., Wines, R., Coker-Schwimmer, E., Rosen, D., Sista, P., & Lohr, K. (2012). Interventions to improve adherence to self-administered medications for chronic diseases in the United States: a systematic review. Ann Intern Med, 157(11).
Walsh, C., Cahir, C., Tecklenborg, S. C., Byrne, C., Culbertson, M. R., & Bennett, K. (2019). The association between medication non-adherence and adverse health outcomes in ageing populations: A systematic review and meta-analysis. British Journal of Clinical Pharmacology, 85(11), 2464–2478. https://doi.org/10.1111/bcp.14075
IMAGE CREDIT: A_STOCKPHOTO/SHUTTERSTOCK.COM

