

From Strategy to Structure: Developing a Heart Failure Care Management Program
BY , RN, BSN, CCM
Heart failure represents a significant national health crisis, accounting for more than one million hospitalizations annually in the United States. The condition affects approximately one in four individuals over their lifetime, with the prevalence expected to increase from 6.7 million Americans today to 8.5 million by 2030. Notably, heart failure-related mortality has risen steadily each year since 2012.
Nationally, heart failure is among the leading causes of hospitalization for older adults and contributed to more than 425,000 deaths in 2022. Hospitalizations related to heart failure are frequently recurrent, with approximately 25% of patients readmitted within 30 days of discharge. In 2020, direct medical costs associated with heart failure were estimated at $30.7 billion, with projected costs expected to exceed $70 billion by 2030, underscoring the growing financial and quality burden of this condition.
In 2023 IHA Trinity Health Medical Group wanted to establish a proactive approach to working with our heart failure patients, getting to them before they were going to the ED or hospital. We developed a report of all of our heart failure patients over the age of sixty-five who had not seen a cardiologist in greater than 6 months and had other chronic conditions. We assigned them to our care managers to engage in the care management program over 7 months, providing them with a prescriptive list of things that they had to do such as education, medication reconciliation and facilitating a cardiology visit. We enrolled 23% of the patients for a brief time of intervention. After identifying that many patients were not receiving cardiology follow-up after their initial diagnosis or most recent heart failure exacerbation, we engaged with our cardiology partners to better understand their follow-up processes and expectations for this patient population. Together, we also explored ways to address barriers to care and improve access for this population. This has led us to look at our heart failure education, leading us to review and standardize it across the inpatient and ambulatory setting, including our home care as well.
ANALYZE THE DATA
Analysis of IHA utilization data revealed that 20–35% of patients with an initial heart failure admission were readmitted for heart failure within 30–60 days, contributing to a disproportionate share of avoidable costs. Nearly 45% of preventable hospitalizations across IHA were attributable to heart failure, representing a significant driver of inpatient spend and utilization. In the context of value-based reimbursement models—where financial performance is closely tied to cost containment, readmission rates, and quality outcomes—these patterns highlighted the substantial financial risk associated with unmanaged heart failure populations. The findings further demonstrated that physician-led care alone is insufficient to deliver the education, monitoring, and intervention required to reduce utilization, necessitating a more comprehensive, multidisciplinary approach to mitigate costs and improve performance under value-based contracts.
The care management and population health teams analyzed barriers that they identified as they worked with this population, to identify some areas to focus on. We identified the following as our top five barriers:
- Disease knowledge and Understanding: some reported they were not even aware they had heart failure
- Tools for managing health
- Medication: did they understand their medications and were they on the right medications
- Lifestyle and Behavioral Health
- Patient and Caregiver skillsets
DEVELOPING THE HEART FAILURE CARE MANAGER ROLE
This pilot prompted us to reassess our approach and develop a more intentional, focused strategy for serving this population. While we already had 40 care managers engaged with these patients, our goal was to standardize and formalize efforts into a comprehensive, structured program that ensured consistency, quality, and measurable outcomes. Central to this initiative was a commitment to empowering patients and their caregivers with the knowledge, tools, and skills necessary to effectively manage complex chronic conditions. Equally important was the development of an evidence-based outreach model grounded in relationship-building, trust, and open communication, enabling patients to engage honestly without fear of judgment. Given the advanced age and clinical complexity of this population, we also recognized the critical role of family members and support systems. By actively involving caregivers, we aimed to enhance self-care behaviors, improve care coordination, and ultimately elevate patients’ overall quality of life
We took the learnings from the proactive outreach program and prioritized some of the important things we wanted to establish for the program:
- Using our standard heart failure education more effectively.
- Developing smartlist that prompted the care manager to address specific things.
- Standard templates that allowed us to track interventions as well as utilization.
- Incorporating dietary counseling and family caregiver involvement for each patient.
- Pharmacist medication reviews to ensure adherence and cost-efficacy.
We broke down the heart failure education into weekly calls supported by evidence-based learning:
- Learners are allowed to digest the information before they are expected to master it.
- Chunk content into small frequent components: it will take 5-7 sessions to get them to move forward.
- Repetition and reinforcement are crucial in moving data from short term to long term memory- thus we do weekly calls.
- Spacing out repetitions rather than in one lump sum and expecting the patient to recall.
The heart failure care manager completed a heart failure assessment and care plan and was able to provide the patient with a heart failure kit that includes equipment to monitor blood pressure and weight as well as the documents to track and report back to the care manager or physician. The program was a 3-month program in which the care manager had weekly contact to provide education and practiced teach-back for 4-6 weeks and then monthly maintenance calls monthly for 2-3 months.
THE DATA
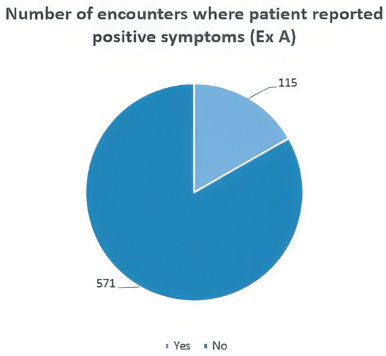
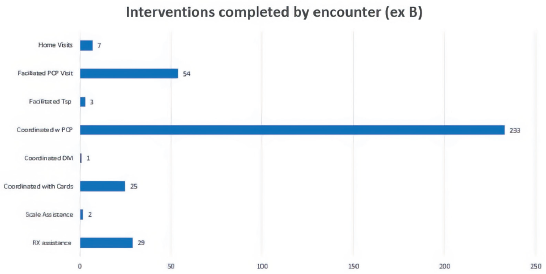
The initial data collected was over 8 months and consisted of utilization of services, symptoms, education, monitoring, referrals, and interventions. We noted that as the care manager was working with the patient there were acute symptoms being reported that required real-time action. We established workflows and processes with the cardiology office to ensure timely actionable management as well as the ability to expedite access to their team (ex A). Through data capture we were able to see where the care manager was focusing efforts through her encounters with the patient (ex B).
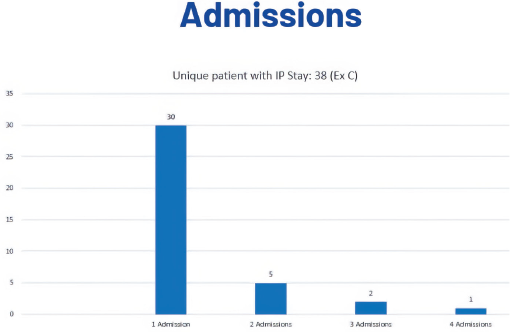
Each encounter the care manager also assessed utilization with the patient, and we were able to use this date to capture emergency room visits and hospitalizations and assess the care manager reported data versus the claims capture. (ex C)
COLLABORATIVE APPROACH WITH PHARMACIST
Effective treatment for heart failure relies on guideline-directed medication therapy (GDMT) and this is where the pharmacist plays a role. Optimal GDMT in the US could prevent 100,000 deaths per year.
We established indicators for referral to Pharmacist:
- Transitions of care patients with 10 medications or more
- Patients that at the time of care management intervention were struggling with medication adherence, whether related to cost or complexity of medications
- Patients that are not currently on a GDMT
- Patients that were experiencing uncontrolled HTN or Diabetes that would benefit from medication modifications
- Patients required intense medication modifications between visits could be referred by cardiology.
LESSONS LEARNED
- As we started to look at the date we identified different interventions and referrals that we felt were important to track and so throughout the process we made modifications.
- Cadence of calls was imperative to maintain relationships with patients, providing better engagement
- When patients were re-admitted to the hospital we had to restart the pathways, specifically if the admission was related to heart failure. It allows us to really focus on symptom identification and teach back with the patient or caregiver.
OUTCOMES
As we have just finished the first year of the program we are starting to analyze and assess the data that we’ve collected as well as looking at the financial impact that this program has had on our re-admissions. Early findings indicate that patients who are actively engaged in the program are developing a stronger educational foundation, which we anticipate will lead to improved knowledge retention and greater confidence in independently managing their heart failure. Patients have expressed that they are grateful for the acknowledgement from the primary care team; that working with the care manager has been informative and empowering for them. In several cases, patients reported that they were previously unaware of certain diagnosis or risk factors until experiencing the exacerbation.
In addition, we have implemented a perioperative heart failure program for patients undergoing surgery. These patients are referred to a heart failure care manager who conducts proactive outreach prior to surgery, providing education on surgical risks, symptom recognition, and heart failure management. Postoperatively, the care manager conducts two to four follow-up calls over a four-week period to support recovery and reduce complications.
REFERENCES
Heart Failure Society of America (HFSA) Home. (n.d.). http://www.hfsa.org/
Centers for Disease Control and Prevention. (n.d.). About heart failure. Centers for Disease Control and Prevention. http://www.cdc.gov/heart-disease/about/heart-failure.html
American Heart Association: To be a relentless force for a world of longer, healthier lives. www.heart.org. (n.d.). https://www.heart.org/
Jenneve, A., Lorenzo-Villalba, N., Courdier, G., Talha, S., Séverac, F., Zulfiqar, A.-A., Arnold, P., Lang, P., Roul, G., & Andrès, E. (2020). Benefit of ambulatory management of patients with chronic heart failure by protocolized follow-up therapeutic education and Remote Monitoring Solution: An original study in 159 patients. Journal of Clinical Medicine, 9(10), 3106. https://doi.org/10.3390/jcm9103106
Inglis, S. C., Clark, R. A., McAlister, F. A., Ball, J., Lewinter, C., Cullington, D., Stewart, S., & Cleland, J. G. (2010). Structured telephone support or telemonitoring programmes for patients with chronic heart failure. Cochrane Database of Systematic Reviews. https://doi.org/10.1002/14651858.cd007228.pub2
Inglis, S. C., Clark, R. A., Dierckx, R., Prieto-Merino, D., & Cleland, J. G. (2016). Structured telephone support or non-invasive telemonitoring for patients with heart failure. Heart, 103(4), 255–257. https://doi.org/10.1136/heartjnl-2015-309191
Tung, H., Lin, C., Chen, K., Chang, C., Lin, Y., & Chou, C. (2012). Self-management intervention to improve self-care and quality of life in heart failure patients. Congestive Heart Failure, 19(4). https://doi.org/10.1111/chf.12014
Winham BG, Bennet RG, Gottlieb S, Care Management Interventions for Older Patients with Congestive Heart Failure. The American Journal of Managed Care. Vol. 9, No. 6: July 2003:447-461.
Berger, B. A., & Villaume, W. A. (2020). Motivational interviewing for Health Care Professionals: A sensible approach. American Pharmacists Association.
Fraser, K., Perez, R., & Latour, C. (2018). CMSA’s Integrated Case Management: A Manual for case managers by case managers. Springer Publishing Company.
 Heidi Steinhebel, RN, BSN, CCM, is the Senior Associate Director of Care Management at Trinity Health IHA Medical Group. A certified case manager for 27 years, she has played a key role in developing and implementing care management programs across commercial and Medicare populations, including collaborations with McKesson and the first Medicare care management program. Heidi has been instrumental in building interdisciplinary care teams—integrating dietitians, pharmacists, and specialty care managers—to support population health and to advance team-based care in the ambulatory setting. Heidi has presented at CMSA National Conferences, NJ End of Life Conferences and has been published on CMSA blog. She is an active leader within the CMSA Detroit Chapter, serving as past secretary and current Director and Education Committee Chair.
Heidi Steinhebel, RN, BSN, CCM, is the Senior Associate Director of Care Management at Trinity Health IHA Medical Group. A certified case manager for 27 years, she has played a key role in developing and implementing care management programs across commercial and Medicare populations, including collaborations with McKesson and the first Medicare care management program. Heidi has been instrumental in building interdisciplinary care teams—integrating dietitians, pharmacists, and specialty care managers—to support population health and to advance team-based care in the ambulatory setting. Heidi has presented at CMSA National Conferences, NJ End of Life Conferences and has been published on CMSA blog. She is an active leader within the CMSA Detroit Chapter, serving as past secretary and current Director and Education Committee Chair.
Trinity Health IHA Medical Group is a non-profit multi-specialty physician group in Michigan. It has over 1000 providers and 170+ primary care and specialty offices, serving over 500,000 patients with a focus on preventative care and extensive, patient-centered services.



