
Resilience Is Not a Buzzword: It’s a Practice
The Problem With "Toughness Culture"
BY , RN, BSN, CCM AND
“I can’t thank you enough for picking up that extra project; I know how busy you are.” “Wow, you’re working overtime this week, too? You’re so committed to your job!” These phrases, praiseworthy in nature, highlight the irony many health professionals frequently feel. In a profession where toughness is synonymous with strength, repeated signs of going above and beyond, pushing through the exhaustion, and staying late shift after shift to document are often viewed as signs of commitment rather than a barely waving ragged caution flag of burnout and self-sacrifice. While it is important to give of ourselves to those we care for, we preach “you can’t pour from an empty cup” to our patients all while gritting our teeth and overextending ourselves, over time draining the essence of empathy and compassion, degrading our usefulness.
Toughness culture is the problem, and this misunderstanding of resilience erodes our own personal well-being and demeans the impact we might have on our patients. Resilience isn’t merely about enduring the difficult—rather, it is the intentional practice to recognize our limitations and the courage to model recovery within systems that often forget it (Sheikhrabori et al., 2022). When we continuously ignore signals that should be telling us we need recovery, we don’t get resilience; the result is resistance.
RETHINKING RESILIENCE: RECOVERY, NOT RESISTANCE
As healthcare workers we are often sold a version of resistance masquerading as resilience. Difficult cases mold us into being coordinators of emotional and psychosocial stability, often while we feel our own boundaries are coming apart at the seams. We listen, tender hearts filled with compassion for our patients’ needs and struggles. We are a sounding board when they seek direction and guidance, providing constant stability between the intersection of physical needs and psychosocial disparities. Over time these can compound, creating the unintended consequence of vicarious trauma—potentially placing clinical judgment in question (Wu et al., 2025).
Resistance can occur when organizational inefficiencies encounter psychologically exhausted case managers. For example, the coronavirus epidemic taught us constantly staying extra and filling in due to staffing shortages, working despite not having enough equipment to do our job safely, and having to daily abandon self-preservation tactics and altruistically care for the good of others while under unthinkable stress- this did not create resilience, it created resistance (Subramanian et al., 2023). While all problems are not the cause of organizational inefficiencies, true resilience is based on how well we recover, not merely our capacity to tolerate endless stress. A resilient case manager doesn’t feel less; they restore more. Equating resilience with resistance perpetuates rewarding unhealthy patterns that often result in burnout. The goal is to shift ourselves from a place where we are merely trying to endure stress and pressure into a familiar, intentional pattern of restorative resilience. In a field where the workplace can be filled with relentless demands and emotional intensity, our mental health is screaming for the space that supports recovery and replenishes depleted resources so that sustained performance remains possible over time.
THE NEUROSCIENCE OF STRESS AND RESET: ENERGY, FOCUS, CONNECTION, BOUNDARIES, MOOD
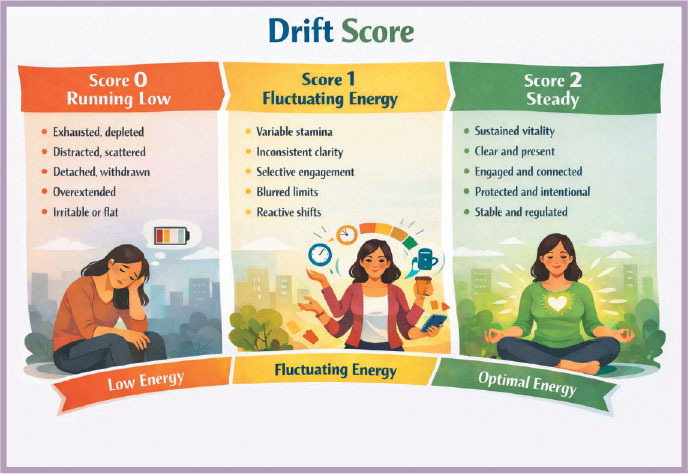
When most people think about burnout, they imagine a sudden collapse. In reality it’s a drift- slow, quiet, and hard to notice- until you’re already running on fumes. The Drift Score was born from that truth. It’s a five-point self-check built to catch early signs of mental and emotional detachment before they become something bigger (Zenian, 2025) . The framework is simple: Energy, Focus, Connection, Boundaries, and Mood. Each rated from 0 to 2, where 0 means you’re running low and 2 means you’re steady. The goal isn’t perfection or even a “high score.” What matters is trend awareness and noticing which direction you’re heading so you can course-correct early.
Correction happens through three levers: Body, Environment, and Connection.
Move your body, even briefly, by stretching, walking, or hydrating to reset your nervous system. Shift your environment by clearing clutter or changing your physical space. Then, reach for connection with a real conversation instead of another email thread. From a neuroscience standpoint, these levers target the body’s natural stress response. Physical movement releases tension and reactivates dopamine pathways that improve motivation. Changing environments interrupts cognitive fatigue, signaling the brain to reset focus. Human connection lowers cortisol levels and restores the oxytocin that helps us feel safe and engaged. Resilience isn’t about toughness or endurance. It’s about rhythm, the natural balance between stress and recovery, focus and reset.
BUILDING MICRO-PRACTICES: BREATHING, REFLECTION, CONNECTION
Micro-practices such as breathing, reflection, and connection remind the brain and body that safety and recovery are always available, even in high-demand roles. Research on mindfulness and stress regulation shows that brief, intentional practices can improve attention, emotional regulation, and resilience when integrated into daily routines rather than separated from work tasks (Kabat-Zinn, 2003). The Drift Score makes this actionable by translating invisible stress signals into something teams can notice, name, and respond to during the workday.
Rather than asking employees to self-identify burnout after it occurs, the Drift Score provides a shared language for recognizing early signs of drift, including reduced focus, emotional disengagement, or reactive communication. For example, a remote team may begin a weekly check-in by briefly rating their Drift Score on a simple scale. When scores trend lower, leaders adjust workload expectations, clarify priorities, or create moments for reconnection. Over time, leaders identify patterns, and teams learn that drift is not a personal failure but a signal to recalibrate.
The Drift Score is not a wellness program. It is a leadership tool that embeds awareness into everyday work, helping remote teams remain present, productive, and human in the modern workplace.
THE ROLE OF ORGANIZATIONAL SUPPORT
Care managers and healthcare professionals can work on restoration and resilience within the personal confines of their own lives, but when the system they exist in rewards overworking and depletion, they will ultimately burn out anyway. Organizational support is imperative in true resilience; it creates the safe space necessary to facilitate difficult conversations. Rather than an organization demanding its employees to “push through”, resilience champions balance psychological safety with difficult truths. There must be a safe place for employees to debrief, express concerns, hash out quality issues, and solicit solutions. The support of an organization makes resilience possible as it permits recovery to be built into its systems.
Organizations that recognize the value of prescribed mental health days can strengthen resilience in professional practice by thoughtfully designing PTO structures that encourage restorative time off, while avoiding incentives that unintentionally normalize unhealthy and unsustainable work patterns. When approached with an understanding of operational demands and the need to maintain continuity of care, these policies can align leadership behaviors with practical solutions that support both staff well-being and the stability of the healthcare system. Addressing cognitive dissonance requires organizational support to help translate conceptual ideas into sustainable workplace practices that contribute to a resilient culture. These considerations highlight the importance of examining resilience through a shared lens, one that includes not only individual experiences but also the operational realities leaders must navigate to sustain the healthcare continuum without inadvertently increasing workload pressures that contribute to burnout.
FROM DEPLETION TO RESTORATION: A PRACTICAL ROADMAP
First, the organization and employees must be willing to partner together. There must be a shared vision to recognize signs of depletion, such as irritability and inward emotional withdrawal. Dreading shifts and patient/member interactions before one even begins working is a sure sign of burnout. Ignoring signs of emotional blunting and numbness can quickly morph us into less empathetic case managers; checking boxes and task-focused rather than engaging as patient/member-centered, individualized and efficient, emotionally intelligent conversationalists who empower and create lifelong positive changes.
The turning point must be when we can recognize that our compassion, poise and presence, or clinical judgement are compromised, and we partner with one another to delve into those micro-practices of restoration. When we can name what is heavy and difficult in the workplace and create a safe place to navigate and inspire change, we are protecting the part of us that belongs to our nervous system, not merely our productivity metrics. When we listen to our bodies and label the signs of stress and defeat, roadblocks become roadmaps.
Starting the process can be simple action such as blocking off your calendar for your entire lunch and moving away from your desk or work area. After a morally or emotionally traumatic call or visit, giving yourself permission to process this with a short reset. Taking the time to intentionally message your supervisor or a trusted colleague and admit, “that was a lot”. Other activities could include journaling a bit about your feelings, praying, incorporating some box breathing techniques, and learning to “be okay” with sitting with the uncomfortable for a few moments enough to process the difficult rather than immediately push it away. Advocate for yourself and your colleagues in your organization to create emotionally and mentally safe places where these intentional micro-practices restore compassion and carve out deliberate and effective coping mechanisms and new patterns of change.
A CALL TO ACTION: RESILIENCE RESET
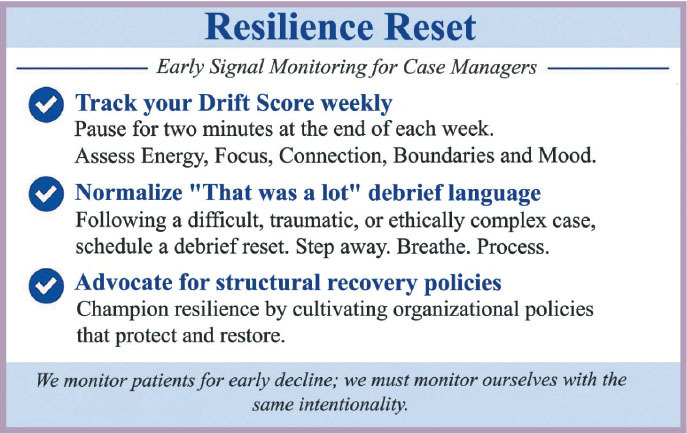
Organizations may consider using a tool such as Resilience Reset to catalyze the opportunity to reframe and reprioritize resilience within teams. By using the checkpoint action items listed in figure 2 as a guide, teams can track Drift Scores weekly, normalizing the place and language to cultivate an environment to process and debrief difficult cases. Leaders can implement team-building dialogue grounded in motivational interviewing techniques such as affirmation and reflection. Naming the difficult, spending a moment to process as a group the shared emotional experience- these actions, when deliberate, honest, and unbiased, can quickly spur feelings of validation. When we can exist in one another’s framework we can work together towards a solution. The Resilience Reset turns emotionally exhausted case managers into resilience champions, and as they gain confidence in the restoration power resilience offers, structural policies can be revisited and reimagined. We monitor our patients for early decline; we must monitor ourselves with the same intentionality. The Resilience Reset can assist teams in the development of resilience, where it becomes more than a buzzword, resilience becomes a practice.
RESILIENCE IS A SHARED RESPONSIBILITY
Resilience isn’t something you are born with; resilience is created by relational and systemic outcomes and is directly proportional to the interactions and motives between the individual employee, the team, and the organization. Teams have the option to reinforce toughness culture or to foster a reality of resilience. Recognizing our own personal depletion tendencies, enacting realistic boundaries, and instilling micro-practices like breathing, reflection, and connection that help the nervous system reset produces personal and organizational accountability and pride. However, resilience cannot rely solely on individual coping strategies when professionals face ongoing stressors— whether stemming from organizational demands, the inherent emotional burden of the work, or external pressures such as vicarious trauma or unsafe staffing—and is most effective when responsibility is shared. Because true resilience isn’t built by tougher people, but by braver systems and partnerships who remind us that it’s not just about surviving the workload but sustaining the people who accomplish it.
REFERENCES
Kabat-Zinn, J. (2003). Mindfulness-based interventions in context: Past, present, and future. Clinical Psychology: Science and Practice, 10(2), 144–156. https://doi.org/10.1093/clipsy.bpg016
Sheikhrabori, A., Peyrovi, H., & Khankeh, H. (2022). The main features of resilience in healthcare providers: A scoping review. Medical Journal of the Islamic Republic of Iran, 36(1), 3. https://doi.org/10.47176/mjiri.36.3
Subramanian, K., Chandrasekaran, V., Monica Jasmin, A. R., Muthuramalingam, A., & Govind, P. (2023). The effect of covid pandemic on human resilience and recovery. Journal of Current Research in Scientific Medicine, 9(1), 5–10. https://doi.org/10.4103/jcrsm.jcrsm_94_22
Wu, Y., Liu, Y., Bo, E. et al. “Falling in and climbing out”: a qualitative study on vicarious trauma among hospice nurses (2025). BMC Nurs 24, 1320 https://doi.org/10.1186/s12912-025-03845-9
Zenian, A. (2025). 5 ways to prevent remote workers from drifting. Entrepreneur. https://www.entrepreneur.com/living/5-ways-to-prevent-remote-workers-fromdrifting/343910
 Amanda Leigh Law, BSN, RN, CCM, is a Senior Learning & Development Specialist in Central Arkansas. She brings clinical and case management expertise in transitions of care, member engagement, and professional education. Amanda designs training programs that promote evidencebased practices and resilience among care managers. She lives in Heber Springs, Arkansas with her husband and two children, where she enjoys homesteading, sourdough baking, and building a warm community around lifelong learning.
Amanda Leigh Law, BSN, RN, CCM, is a Senior Learning & Development Specialist in Central Arkansas. She brings clinical and case management expertise in transitions of care, member engagement, and professional education. Amanda designs training programs that promote evidencebased practices and resilience among care managers. She lives in Heber Springs, Arkansas with her husband and two children, where she enjoys homesteading, sourdough baking, and building a warm community around lifelong learning.
 Haseen Williams is a Senior Learning & Development Specialist in Southern California. He serves as a New Hire Trainer for Care Management staff, supporting the development of clinical competencies and operational excellence within care management teams. Haseen focuses on equipping new professionals with the foundational skills, organizational knowledge, and structured training necessary to succeed in complex healthcare environments. He is a dedicated family man with a passion for coaching high school girls’ basketball.
Haseen Williams is a Senior Learning & Development Specialist in Southern California. He serves as a New Hire Trainer for Care Management staff, supporting the development of clinical competencies and operational excellence within care management teams. Haseen focuses on equipping new professionals with the foundational skills, organizational knowledge, and structured training necessary to succeed in complex healthcare environments. He is a dedicated family man with a passion for coaching high school girls’ basketball.


