

Bridging Adolescence and Adulthood: Case Management for Transitional-Age Young Adults
BY , MSN, RN, BCPA, CPC
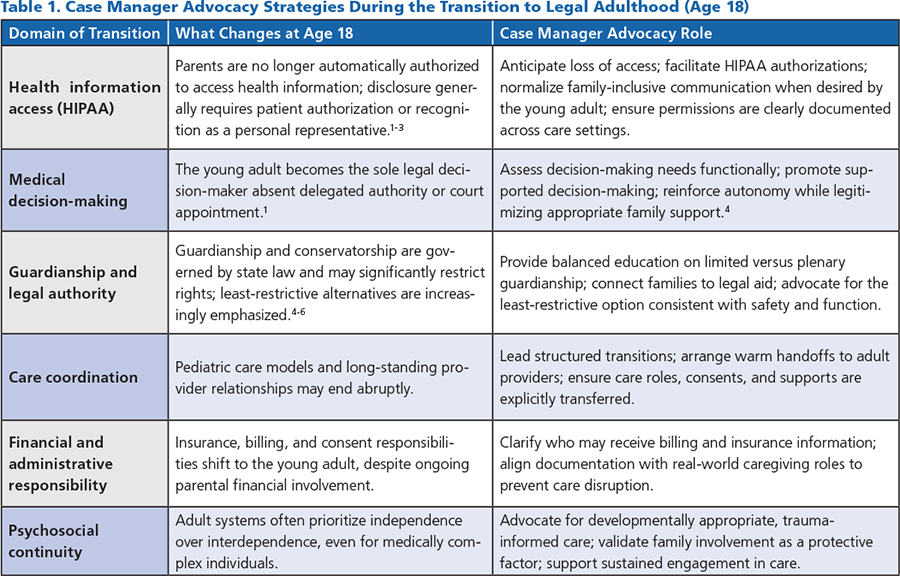
A child’s eighteenth birthday marks an abrupt and consequential transition, not only socially but legally, transforming a dependent minor into an autonomous adult overnight. In healthcare, this legal reclassification can fracture continuity of care, abruptly limiting parental access to medical information, decision-making authority, and coordination roles that have often been essential for managing complex, chronic, or rare conditions. Families who have functioned as integral caregivers may suddenly find themselves excluded by privacy statutes, consent requirements, and adult-oriented healthcare systems. Parental support remains indispensable for many young adults with complex medical needs, neurodevelopmental differences, or significant functional limitations. This legal-clinical disconnect creates profound challenges in care coordination, advocacy, and outcomes.
Case managers are uniquely positioned to serve as stabilizing advocates, bridging legal realities, clinical needs, and family dynamics at the precise moment when systems tend to fracture. As young patients age into legal adulthood, case managers can proactively help families anticipate and navigate the implications of federal and state policies, including the loss of automatic parental access under the Health Insurance Portability and Accountability Act (HIPAA). Beyond education, effective case management requires active facilitation: normalizing continued parental involvement when clinically appropriate, helping young adults articulate consent preferences, and coordinating interdisciplinary teams that honor autonomy while preserving safety, advocacy, and continuity of care.
Reframing parents not as barriers to independence but as essential partners in care, case managers can mitigate care disruption, reduce administrative burdens, and ensure that medically complex young adults do not lose critical support simply because they have reached a legal threshold that does not reflect their lived reality.
Turning eighteen for students with complex chronic conditions can also include a transition to college which introduces a second, often unrecognized, care transition, learning to live independently while managing health needs in systems not designed for medical complexity. Case managers play a critical advocacy role in helping students and families anticipate accommodations that support both health and academic success, including accessible housing, medical parking permits, flexible attendance policies, exam modifications, emotional support animal requirements…all of which require coordination with campus disability and health services. Equally important is supporting the gradual shift of responsibilities helping students build self-advocacy skills while maintaining appropriate parental involvement as a safety net. Without the help of case managers and intentional planning, the demands of independent living can jeopardize health stability, educational engagement, and long-term outcomes.
As healthcare, education, and legal systems continue to define adulthood by age rather than functional need, case managers remain essential advocates for continuity, equity, and patient-centered care. By anticipating legal transitions, elevating family/caregiver partnerships, and supporting young adults in developing self-advocacy skills, case managers help prevent avoidable gaps in care during some of the most vulnerable transitions of life. Advocacy at these intersections is not ancillary to case management practice, it is foundational. Ensuring that young adults with complex conditions are supported, heard, and protected is central to achieving sustainable outcomes across their lifespan.
REFERENCES
- U.S. Department of Health & Human Services. Personal representatives under the HIPAA Privacy Rule. Updated January 5, 2024. Accessed February 27, 2026. https://www.hhs.gov/hipaa/for-professionals/privacy/guidance/personal-representatives/index.html
- Code of Federal Regulations. 45 CFR § 164.502. Uses and disclosures of protected health information. Accessed February 27, 2026. https://www.ecfr.gov/current/title-45/subtitle-A/subchapter-C/part-164/subpart-E/section-164.502
- Code of Federal Regulations. 45 CFR § 164.508. Uses and disclosures requiring authorization. Accessed February 27, 2026. https://www.ecfr.gov/current/title-45/subtitle-A/subchapter-C/part-164/subpart-E/section-164.508
- Kohn NA, Blumenthal JA, Campbell AT. Supported decision-making: A viable alternative to guardianship? Dickinson Law Rev. 2013;117(4):11111157.
- U.S. Department of Justice, Elder Justice Initiative. Guardianship: Less restrictive options. Updated September 30, 2024. Accessed February 27, 2026. https://www.justice.gov/elderjustice/guardianship-less-restrictive-options
- Virginia Code § 64.22000. Guardianship and conservatorship definitions. Accessed February 27, 2026. https://law.lis.virginia.gov/vacode/title64.2/chapter20/section64.2-2000/
 Heather Kelly, MSN, RN, BCPA, CPC, is a registered nurse with more than 30 years of healthcare experience, including oncology, hospice and palliative care, and healthcare administration. She brings a strong background in care coordination, medical policy, and clinical program strategy, with a focus on improving access, quality, and patient centered outcomes. Heather currently serves as a Senior Clinical Strategist, collaborating with multidisciplinary teams to support effective care management and program development. She is a frequent community speaker on cancer survivorship and end of life planning and is deeply committed to patient advocacy and professional mentorship.
Heather Kelly, MSN, RN, BCPA, CPC, is a registered nurse with more than 30 years of healthcare experience, including oncology, hospice and palliative care, and healthcare administration. She brings a strong background in care coordination, medical policy, and clinical program strategy, with a focus on improving access, quality, and patient centered outcomes. Heather currently serves as a Senior Clinical Strategist, collaborating with multidisciplinary teams to support effective care management and program development. She is a frequent community speaker on cancer survivorship and end of life planning and is deeply committed to patient advocacy and professional mentorship.

